Search the hub
Showing results for tags 'Organisational learning'.
Found 551 results
-
Content Article
.png.3147e7fdf0a155dba1a75b3244d6c5be.png) In this blog, Katy Fisher, Senior Nurse Quality & Improvement at NHS Professionals, explains how she became involved in Appreciative Inquiry and asks the question: what could Appreciative Governance start to look like in the NHS and what small steps can we all do to achieve that together?
In this blog, Katy Fisher, Senior Nurse Quality & Improvement at NHS Professionals, explains how she became involved in Appreciative Inquiry and asks the question: what could Appreciative Governance start to look like in the NHS and what small steps can we all do to achieve that together? -
Content ArticleCaring Corner is a podcast hosted by Katy Fisher and Kayleigh Barnett sharing real stories of Appreciative inquiry in health and care.
-
Content Article
 The original National Safety Standards for Invasive Procedures (NatSSIPs) were published in 2015. In 2023 the standards were revised (NatSSIPs 2) with the Centre for Perioperative Care (CPOC), with a focus on bolstering of the organisational standards (people, processes and performance) in addition to the sequential steps that teams follow. The standards are intended to share the learning and best practice to support multidisciplinary teams and organisations to deliver safer care. Patient Safety Learning spoke to Annie Hunningher and Claire Morgan about the changes to the revised NatSSIPs 2, how NatSSIPs 2 is being implemented and what more needs to be done to promote and engage leadership for action.
The original National Safety Standards for Invasive Procedures (NatSSIPs) were published in 2015. In 2023 the standards were revised (NatSSIPs 2) with the Centre for Perioperative Care (CPOC), with a focus on bolstering of the organisational standards (people, processes and performance) in addition to the sequential steps that teams follow. The standards are intended to share the learning and best practice to support multidisciplinary teams and organisations to deliver safer care. Patient Safety Learning spoke to Annie Hunningher and Claire Morgan about the changes to the revised NatSSIPs 2, how NatSSIPs 2 is being implemented and what more needs to be done to promote and engage leadership for action. -
News Article
‘Burdensome’ patient safety inquiries taking up too much time, says NHSE chief

Patient Safety Learning posted a news article in News
NHS England’s head of patient safety has suggested too much time and resource is being spent on “burdensome” inquiries to investigate failings in the system. Aidan Fowler said national chiefs want to see a shift away from “looking back 10 years and asking ‘what did we miss’”, and instead wants teams to be resolving problems in real time. At trusts where safety concerns have been highlighted, he said “people descend, and there are a lot of asks, and the pressure mounts, and they end up with an action list of hundreds of things, and it becomes very burdensome – we have to avoid that”. Speaking at a session at the NHS Confederation Expo event in Manchester this week, he encouraged organisations to report concerns early so NHSE can respond more quickly, supporting them and working through problems to prevent public inquiries from needing to happen in the first place. Mr Fowler added: “We have to get more proactive. We will spend less of our time in the future, is the plan, than we are now – doing what I call driving in the rear view mirror. “We don’t want to be looking back 10 years and asking, ‘what did we miss’, we want to be seeing things in real time… we don’t want to be spending our time in big inquiries into failings in the system.” Read full story (paywalled) Source: HSJ, 14 June 2024 -
Content ArticleThis template standardises the reporting of After Action Reviews (AARs). It is not intended to be an AAR facilitation guide. The template has been co-designed with staff leading AARs in a range of healthcare organisations. The structure is purposefully simple so that AARs can focus on reflective conversation and do not become a bureaucratic documentation exercise. This structure will continue to be evaluated and developed by the National Patient Safety Team. It can be downloaded from the attachment below or it's available on FutureNHS within the AAR tool space here: https://future.nhs.uk/NHSps/view?objectId=42826256
-
Content Article
Lessons not learned: A family's lengthy efforts to turn complaints into improvements

Anonymous posted an article in PHSO investigations
 A family describe the lengthy efforts they had to take to try to ensure their complaints about their loved one's end of life care would result in improvements at the hospital.
A family describe the lengthy efforts they had to take to try to ensure their complaints about their loved one's end of life care would result in improvements at the hospital.- Posted
- 1 comment
-
- (and 11 more)
-
EventThis training will support the development of expert understanding and oversight of systems based patient safety incident response throughout the healthcare system - in line with NHS guidance, based upon national and internationally recognised good practice. This course covers the end-to-end systems-based patient safety incident response based upon the new NHS PSIRF and includes: PSIRF and associated documents (PSIRP, PSII standards) oversight framework effective oversight and supporting processes related to incident response maintaining an open, transparent, and improvement focused culture importance of communication and involvement of those affected (preventing further harm) commissioning and planning of patient safety incident investigations complex investigations spanning different organisational, care setting, and stakeholder boundaries. WHO SHOULD ATTEND Executives, commissioning, & service managers supporting service lead investigator roles. The following only after attending the 2-day systems approach to patient safety incident response: All Executive, Commissioner and Service Leads for investigation; All Lead investigators conducting patient safety incident investigations investigators conducting. Register hub members receive a 20% discount. Email info@pslhub.org for discount code.
-
EventTraining to support the development of expertise involving patients, families, carers and staff when things go wrong, in line with NHS guidance, based upon national and internationally recognised good practice. To include the duty of candour and ‘being open’ principles. This course covers the end-to-end systems-based patient safety incident response based upon the new NHS PSIRF and includes: Duty of candour regulations. Being open and apologising when things go wrong. Challenges/complexities associated with cases where there is more than one investigation. Effective communication, including dealing with conflict and difficult conversations. Effective involvement of those affected by a patient safety incident throughout the incident response process to ensure a thorough and richer investigation. Sharing findings. Signposting and support: including loss, trauma and stress. WHO SHOULD ATTEND Lead investigators conducting patient safety incident investigations. Executive and service lead for duty of candour. Executive and service lead for patient safety. Executive and service lead for the supporting response to patient safety incidents. Investigators supporting patient safety incident investigations. Register hub members receive a 20% discount. Email info@pslhub.org for discount code.
-
Content Article
 In the past, long before Covid, doctors used to openly discuss complex cases and unexpected deaths on an anonymous basis either in the doctors' mess or in medical grand rounds hosted by their hospital’s clinical education department. What's happened to these forums for learning? Are these clinical conversations alive and well, and helping doctors and nurses alike to learn from safety incidents? Or have medical grand rounds disappeared from practice?
In the past, long before Covid, doctors used to openly discuss complex cases and unexpected deaths on an anonymous basis either in the doctors' mess or in medical grand rounds hosted by their hospital’s clinical education department. What's happened to these forums for learning? Are these clinical conversations alive and well, and helping doctors and nurses alike to learn from safety incidents? Or have medical grand rounds disappeared from practice?- Posted
- 2 comments
-
- (and 3 more)
-
Content ArticleSuicide and non-fatal self-harm represent key patient safety events in mental healthcare services. However, examples of optimal practice that help to keep patients safe also often important learning for organisations and healthcare professionals. This study in BMC Psychiatry aimed to explore clinicians’ views of what constitutes good practice in mental healthcare services in the context of suicide prevention. The study highlighted clinicians’ views on good practice specific to mental health services that focus on enhancing patient safety via prevention of self-harm and suicide. The authors concluded that clinicians possess important understanding of optimal practice, but there are few opportunities to share such insight on a broader scale. A further challenge is to implement optimal practice into routine, daily care to improve patient safety and reduce suicide risk.
-
Content ArticleThis report by the Maternity & Newborn Safety Investigations (MNSI) programme examines findings from 92 of their investigations where safety recommendations were made to midwife-led units in NHS hospital trusts in England. It highlights key learnings and prompts to help trusts to consider how safety risks can be mitigated and drive improvements in care.
- Posted
- 1 comment
-
1
-
- (and 4 more)
-
Content Article
 A subjective, biased, and an open ended inquiry into one of the most famous accidents in the maritime history – the capsizing of the Costa Concordia. Nippin Anand's first-hand interviews with the captain followed by a series of workshops around the world gradually became a source of learning and inner change. Read a foreword by Steven Shorrock Buy the book here
A subjective, biased, and an open ended inquiry into one of the most famous accidents in the maritime history – the capsizing of the Costa Concordia. Nippin Anand's first-hand interviews with the captain followed by a series of workshops around the world gradually became a source of learning and inner change. Read a foreword by Steven Shorrock Buy the book here -
Content Article
Appreciative inquiry case study

katy.fisher posted an article in Patient Safety Incident Response Framework (PSIRF)
Appreciative inquiry is one of the Patient Safety Incident Response Framework (PSIRF) tools that can be used to learn from patient safety incidents. Katy Fisher, Senior Nurse Quality & Improvement at NHS Professionals, shares how she designed and introduced an appreciative inquiry tool at her hospital.- Posted
- 2 comments
-
1
-
- (and 4 more)
-
Content ArticleOne of the core ambitions of Care Quality Commission is to ensure that the services it regulates have a stronger safety and learning culture. Through their new quality statements, they are looking to assess both ‘safety through learning’ and ‘learning culture’. To ensure they take the best approach to assessing providers on this topic and to ensure they are able to give providers the best quality information on what good looks like in this area, the CQC would like your feedback through this short survey.
-
Content ArticleJudy Walker describes how an After Action Review following a sporting event ensured significant learning took place and led to a worldwide change in first aid training.
-
Content Article
Think Ammonia! Elliot's story
Patient Safety Learning posted an article in Patient stories
In March 2018, Elliot Peters, 14, died after becoming suddenly and seriously ill before being diagnosed with Ornithine transcarbamylase (OTC) deficiency. His mum, Holly, is dedicated to speaking out about Elliot’s story to raise awareness and prevent more deaths. -
Content ArticleAs Rob Behren steps down as the Parliamentary and Health Service Ombudsman (PHSO) he records an episode of Radio Ombudsman, reflecting on his seven years in office. He also tells us about his early life, his career before PHSO and shares his future plans.
-
Content ArticleAlong with the Care Inspectorate, Healthcare Improvement Scotland have established a National hub for reviewing and learning from the deaths of children and young people (National hub). The National hub uses evidence to deliver change. It ultimately aims to help reduce preventable deaths and harm to children and young people.
-
News Article
Health board not learning from preventable deaths
Patient Safety Learning posted a news article in News
Lessons have not been learned to prevent further deaths in north Wales, coroners have told the health secretary. Over the past year, coroners in Wales wrote 41 "prevention of future deaths reports" and more than half were issued to Betsi Cadwaladr health board. Health Secretary, Eluned Morgan, said 27 reports issued since January 2023 was "of significant concern". Betsi Cadwaladr health board said every report was taken very seriously and work was ongoing to respond to key themes. Ms Morgan said all but three of the deaths happened before the health board was moved back into special measures in February 2023. The "systemic issues" that emerge as common themes from the coroners' reports include: the quality of investigations and effectiveness of actions a lack of integrated electronic health records impacting care the impact of delays in the system on ambulance response times. In a written statement earlier this week, Ms Morgan said the health board had given assurances that it was taking the matter "extremely seriously". Read full story Source: BBC News, 21 March 2024 -
Content Article
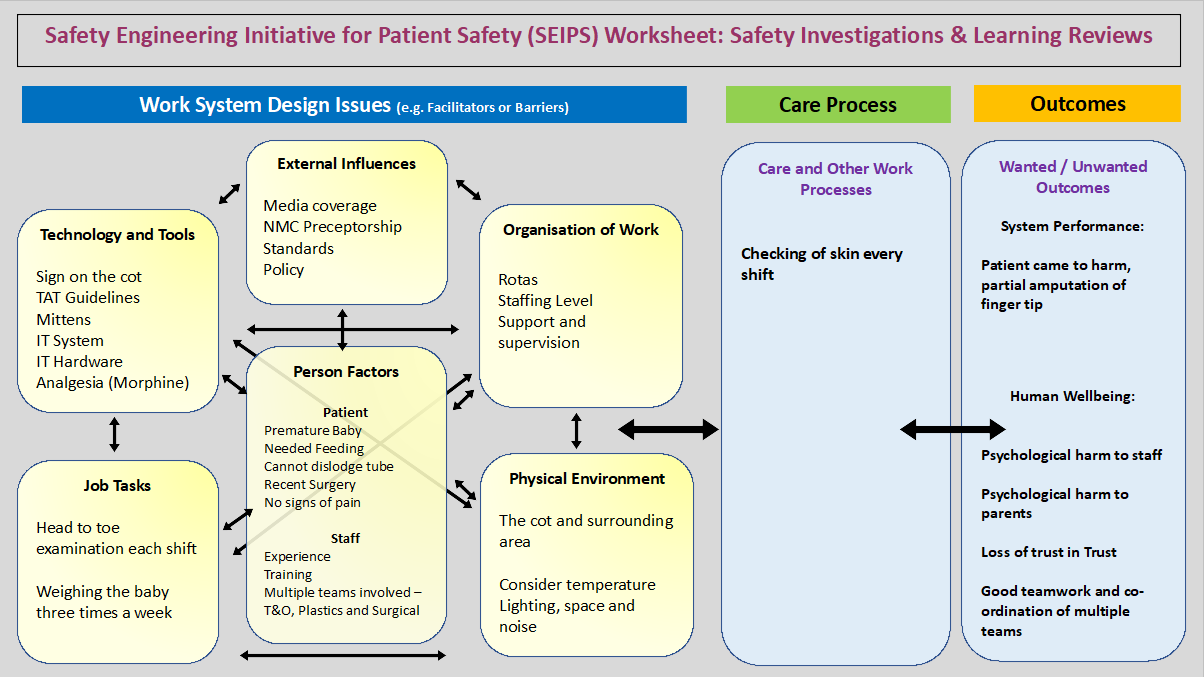 Chris Elston, a patient safety education lead, shares how he used Safety Engineering Initiative for Patient Safety (SEIPS) and Accident Mapping (AcciMap) to learn from a patient safety incident at his Trust.
Chris Elston, a patient safety education lead, shares how he used Safety Engineering Initiative for Patient Safety (SEIPS) and Accident Mapping (AcciMap) to learn from a patient safety incident at his Trust. -
Content ArticleDiagnostic errors cause significant patient harm. The clinician’s ultimate goal is to achieve diagnostic excellence in order to serve patients safely. This can be accomplished by learning from both errors and successes in patient care. However, the extent to which clinicians grow and navigate diagnostic errors and successes in patient care is poorly understood. Clinically experienced hospitalists, who have cared for numerous acutely ill patients, should have great insights from their successes and mistakes to inform others striving for excellence in patient care.
-
Event
Systems approach to learning from patient safety incidents

Sam posted an event in Community Calendar
untilTraining to support the development of core understanding and application of systems-based patient safety incident response throughout the healthcare system - in line with NHS guidance, based upon national and internationally recognised good practice. This course covers the end-to-end systems-based patient safety incident response based upon the new NHS PSIRF and includes: purpose of patient safety incident response framework introduction to complex systems, system thinking and human factors restorative just and learning culture duty of candour involving staff in incident response involving patients, families and carers in incident response improvement science and developing system improvement plans general response techniques interviewing and asking questions conducting observations, understanding work as done systems frameworks response types patient safety investigation planning, analysis and report writing commissioning and oversight of an internal investigation a high-level overview of system-based response tools. Register -
Content ArticleSerious incident management and organisational learning are international patient safety priorities. However, little is known about the quality of suicide investigations and the potential for organisational learning. Suicide risk assessment is acknowledged as a complex phenomenon, particularly in the context of adult community mental health services. Root cause analysis (RCA) is the dominant investigative approach, although the evidence base underpinning RCA is contested, with little attention paid to the patient in context and their cumulative risk over time. This study reviewed research in this area and found that recent literature proposes a Safety-II approach in response to the limitations of RCA.
-
Content ArticleIn this video story, Gaylene tells the story of her hospital stay in 1987 when she was very seriously ill—so ill that her doctors thought she would die. She describes how her wishes not to have her family visit when she looked so unwell were not listened to, which resulted in a traumatic visit for Gaylene, her husband and her four children under the age of 5. She highlights the ongoing impact the event had on her family and the importance of good communication between patients and healthcare staff.
-
Content ArticleThe NHS regularly uses temporary staff to fill gaps in its workforce. This investigation explored the challenges of involving temporary clinical staff (bank only staff, agency staff and locum doctors working within trusts) in local trusts’ patient safety investigations. Trust-level investigations are important because they are a way to identify learning to improve healthcare systems, with the aim of reducing the potential for harm to patients. Identifying learning requires staff to be engaged in an investigation; if temporary staff are not involved, learning may be lost, posing a risk to patient safety. HSSIB identified this risk following analysis of serious incident reports provided by acute and mental health NHS trusts. To explore the issue further, the investigation carried out site visits and engaged with NHS trusts, providers of bank staff, agencies that supply staff to NHS trusts, substantive (permanent) NHS staff, bank and agency staff, and a range of national stakeholders.
.png.3147e7fdf0a155dba1a75b3244d6c5be.png)








